

home >IMPROVEMENT TODAY >Stories > BLOG POST DETAILS
A Community-based Approach to Infant and Young Child Feeding - Chibefwe Rural Health Centre - Zambia
03.16.2015
Team members: Deliven Katambwela Chibinga, Nutritionist (author); Dr. Rosemary R. Mwanza, District Community Medical Officer; Mr. Mangala Benedictus, District QA-QI Coordinator, Mrs. Annie Mwaifunga Chishala, Registered Nurse, Miss. Eness Maila, Nutrition Demonstrator; and other community demonstrators & counselors.
BACKGROUND
Reason for selecting the project
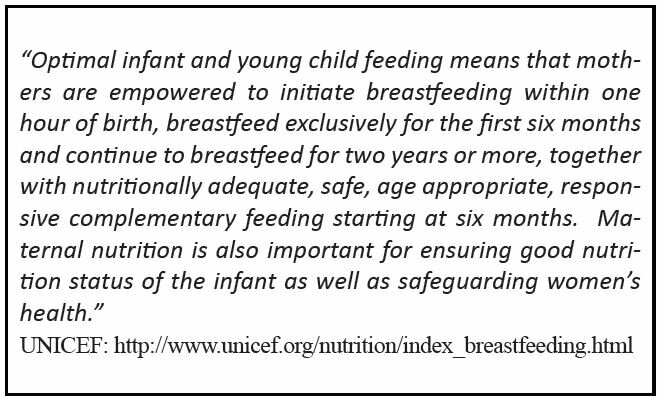
Recognizing the well-documented* significance of infant and young child feeding practices on the health and well being of infants and children, this improvement project focused on helping caregivers acquire knowledge and skills in globally recommended (WHO/UNICEF) feeding practices for children less than two years of age, particularly since nearly 75% of children admitted in the Chibefwe Rural Health Centre’s children’s ward for severe malnutrition were aged 0-23 months.
IMPLEMENTATION PERIOD
In Mkushi District, the project was introduced in 2009 after five members of staff were trained in infant and young child feeding (IYCF) strategies. The project is ongoing.
BASELINE DATA
At project initiation, the five member team and additional community demonstrators and counsellors were trained in infant and young child feeding strategies. The pilot center for this initiative was Chalata. At that time, no community volunteers were involved and no data capturing tools were available to track performance.
Towards the end of 2011, 30 community based volunteers who were trained in IYCF conducted a baseline survey among 2,600 children under two years of age in Chibefwe. The results of the survey showed that 1560 children (60%) were well nourished, 806 children (31%) were moderately malnourished, and 234 children (9%) were severely malnourished.
GOAL
The goal of this project was to initiate outreach and counsel caregivers/mothers of the target population, introduce cooking demonstrations, identify malnourished children early and conduct follow-up. Ultimately, staff determined to reduce the case fatality rate of 200/1000 in 2010 - a goal that was achieved with continued reductions between 2011 and 2014.
INTERVENTIONS
The first meeting between the nutritionist and community based volunteers was held at the beginning of 2012 and an action plan was created. Identity cards were produced at a value of K10 (Ten Kwacha or less than 1 US penny) each to enable community volunteers to move from house to house and conduct a baseline survey. The identity cards were procured by Mkushi District Medical Office and distributed to the community based volunteers. Transport money was paid at K20 (Twenty Kwacha) per day
each for three days to enable volunteers to move to distant catchment areas. Four bicycles were later procured through district grants (community funds) for use by volunteers to reach geographically distant catchment areas (pictured below).
Mentorship and follow-up of the volunteers was conducted by UNICEF, which supported the team by motivating the volunteers with bags, pens, gumboots, raincoats, chitenge materials and T-shirts. Four sets of pots were purchased followed by the initiation of cooking demonstrations.
Infant and young child feeding support groups were formed. Early identification of malnourished children was intensified and referrals were made from the community to the health center.
Two additional posts for growth monitoring and promotion were opened and twenty three additional community volunteers were trained in IYCF.
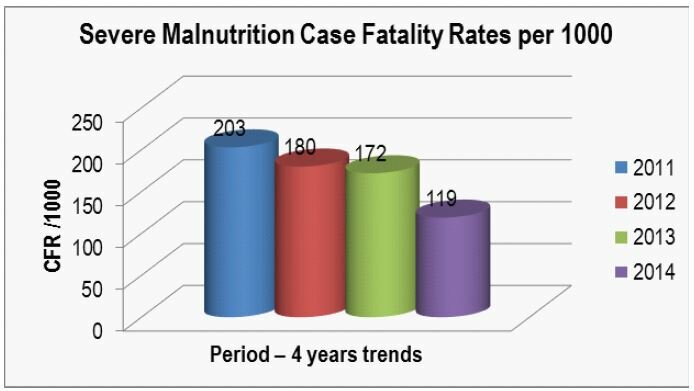
Data demonstrated that rates of malnutrition were rising, even as the case fatality rate was slowing. The IYCF team determined that this could be attributed to more frequent identification of malnourished children because of increased screening. Nonetheless, the severe malnutrition case fatality rate was nearly halved between 2011 and 2014, decreasing from 203/1000 to 119/1000.
Compared to other health centers in the district, Chibefwe appears to be the only center with a significant problem of malnutrition; nutritional activities are much more intensified in this area and malnourished children are rarely missed.
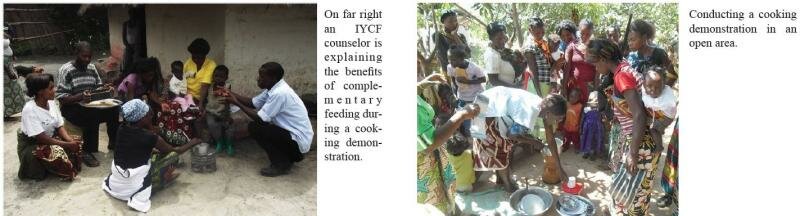
Training of community infant and young child feeding counselors has facilitated introduction of other key nutrition activities. Five cooking demonstration posts have been opened and cooking demonstrations are now occurring (pictured above). The number of growth monitoring posts increased from 12 to 14 in order to bring services closer to families, with routine door to door counseling in IYCF.
CHALLENGES
- Lack of shelters for cooking demonstrations
- Lack of transport to reach distant catchment areas, especially the farm block (subsequently addressed through procurement of bicycles from district grants, as noted.
- Competition of programs, e.g., one volunteer may be involved in various programs and prefer to undertake an activity for which he/she is paid
- Inadequate scales resulting in low growth monitoring data
LESSONS LEARNED
Community volunteers can play a critical role in outreach activities and in identifying malnourished children. Results of this outreach are key to conducting targeted nutrition related activities and eventually reducing mortality in under-5 children.
Motivating volunteers to do work does not require huge sums of money. Moreover, developing local, context-specific interventions that include the community contributes to the potential for programmatic sustainability. For example, knowledge and skills building activities included how to maximize the benefit of locally available foods instead of bringing food into the community at greater cost.
STRATEGIES TO SUSTAIN GAIN
Mentorship of volunteers has been a key activity to ensure ongoing support for learning and sustainability. Further, motivation of community volunteers has been facilitated by provision of low-cost incentives such as t-shirts, transport allowances or capital to finance local income generating activities.
Refresher trainings for volunteers are needed. One training every two years is appropriate and costs about thirty three thousand kwacha (app. 5.50USD) since the district has its own trainers.
Within the last year, eight additional sets of pots were purchased through district grants for cooking demonstrations. A digital camera was procured to facilitate storytelling and knowledge sharing of activities at health facilities and in communities. Finally, and importantly, a nutritionist was trained in IYCF in March 2014 to enhance mentorship of volunteers for this project.
nutrition
Stories
0
Leave A Comment