Background:
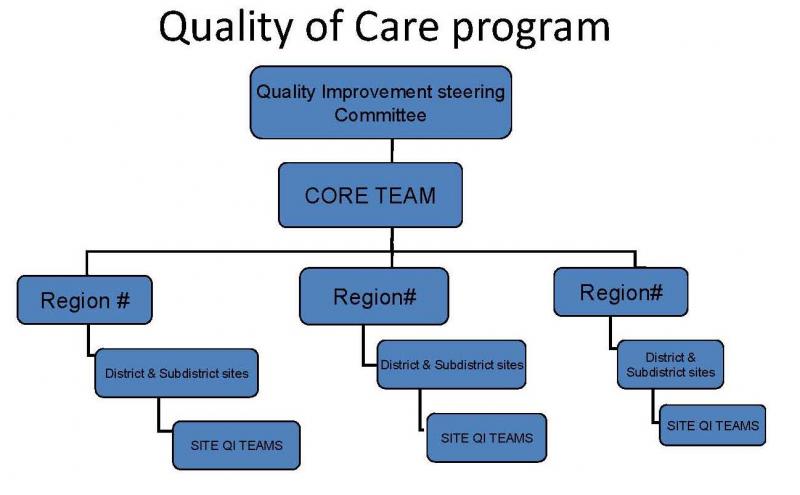
Since roll-out of HIVQUAL-Uganda (HQ-U) in 2006, the program has achieved rapid scale-up from an initial 20 facilities to 127 facilities in 42/87 districts of 12/14 regions. This includes establishment of regional quality improvement (QI) coordination and formation of QI teams at the facility-level. In addition to performance measurement with core adult and pediatric HIV care & treatment indicators, expansion is underway to include prevention-of-mother-to-child-transmission (PMTCT) and HIV counseling and testing indicators.
As of October 2009, the HQ-U in-country team has trained 57 district officers from 25 districts, carried out one joint coaching and mentoring training with the district teams, and submitted district QI reports. The team has facilitated the initiation of an interdepartmental national HIV Quality Steering Committee, and they have successfully developed a national quality plan that encompasses HIV and non-HIV care.
Plans are currently underway to intensify district engagement to support development of district-level implementation plans, integrate QI in district work plans, and continue building capacity for district health teams. Additional district meetings are planned for March, April and May.
HIVQUAL-Uganda had an abstract accepted to the International Conference on Quality and Safety in Nice, France in April 2010.
Demographic Data
- Population: 30 million
- HIV prevalence:
-5.4% general adult population
-135,000 estimated new infections and 77,000 deaths in 2007
-Over 1.1 million infected:
480,000 women
130,000 children under the age of 15 years
- Sexual transmission is the primary mode of transmission (81%) and mother to child (18%)
- TB/HIV prevalence: ~ 60% of TB patients have HIV
- Other pertinent Demographics:
- Year Program Began: Gv’t engagement in 2005 with national rollout in 2006
- Scope: A
- Scope: Adult and pediatric HIV care and treatment with (early stage) of expansion into PMTCT and HCT
- Number of facilities: 20 Pilot sites, now 127 facilities in 42 of 87 districts, and 12 of 14 regions
HIV/AIDS Epidemic
Uganda faced a rapid increase in HIV prevalence in the late 1980’s and early 1990’s. This period was followed by a decline in the infection rate that was largely attributed to delayed sexual debut of young people, reduction in number of sexual partners, and increased condom use. After this decline in the late 1990’s, the prevalence rate has stabilized and was found to be 5.4% in 2007. In 2007, Uganda’s total population was 30,884,000 and there were an estimated 810,000 adults and 130,000 children living with HIV/AIDS. The life expectancy at birth is 50 years. Although the prevalence rate of HIV in Uganda has stabilized in the past decade, HIV prevalence rates still vary based on gender, age, and geography. UNAIDS data states that in 2007 7.5% of women and 5% of men were HIV infected while the rates amongst 15-24 year old women and men is 3.9% and 1.3%, respectively. The HIV prevalence rate in urban areas in 2007 was 10.1% while prevalence in rural areas was about half that, 5.7%.
Uganda Health System Infrastructure:
Uganda has a decentralized system of governance, with local councils at the district and sub-county levels. Local governments maintain political and legislative powers, and jurisdiction over financial and human resources. There are currently 87 districts (97 by July 2010).
The national health system falls under a decentralized model as well, with two national referral hospitals, 14 regional referral hospitals, 100 general hospitals, 166 health center IV’s, 955 health center IIIs, 2006 health center IIs, and village health teams.
In 2007, total ART coverage in Uganda was 31% and 34% of HIV infected women received antiretroviral therapy to reduce the risk of mother-to-child transmission. By the end of 2008, HIV testing and counseling was available in 812 health facilities in the country, up from 554 the previous year.



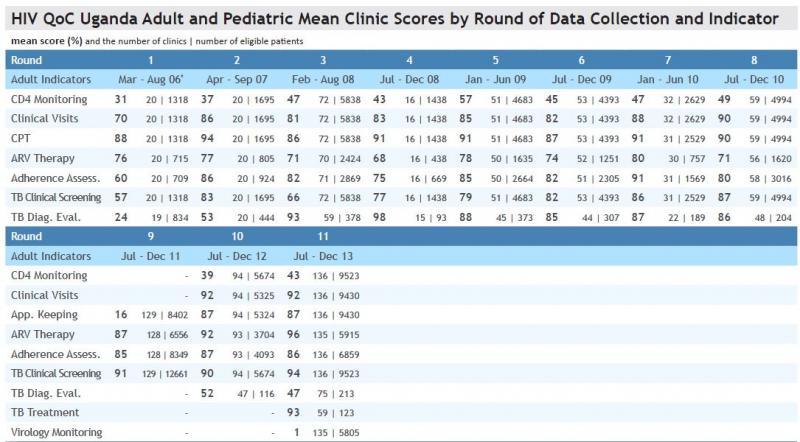
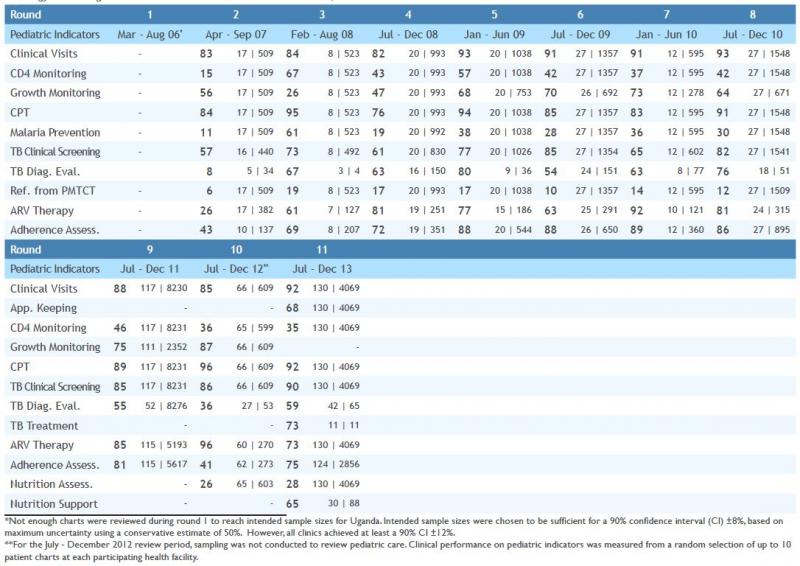
- HQ-Uganda clinics have collected 8 rounds of data reviewing care provided from March 2006 through July 2010.
- 123 clinics have participated in HIVQUAL-Uganda data collection. 101 and 53 clinics have collected at least one round of data reviewing care for adults and children, respectively
- 26,988 adult charts have been sampled from at least 310,894 eligible patients in total across all rounds
- 6,563 pediatric charts have been sampled from at least 22,741 eligible patients in total across all rounds
- Performance rates have been measured for the following 12 indicators: clinical visits, CD4 monitoring, total lymphocyte count, ARV therapy, ART adherence assessment, cotrimoxazole preventive therapy, TB clinical screen, TB diagnostic evaluation, prevention education, malaria prevention, growth monitoring and infant referral from PMTCT